Placing people at significant distances from family and loved ones can be deeply distressing and destabilising for a person’s emotional and mental well-being.
Out-of-area placements continue to be a persistent and serious concern for people and families navigating mental health challenges and complex care needs.
Findings from our latest White Paper survey show that over 40% of respondents were placed more than 50 miles from home, with nearly one in five more than 150 miles away.
Families consistently described the impact of distance as deeply negative, using words like “traumatic,” “isolating,” and “stressful.” Being far from home made it harder for relatives to visit and stay involved in care decisions.
Many also spoke about growing anger, frustration, and a loss of trust in the mental health system following these experiences.
In 2025, England recorded 7,191 new inappropriate out-of-area placements – around 113 each week – including 381 involving children. These figures point to the scale of the issue and the urgency of taking action without delay.
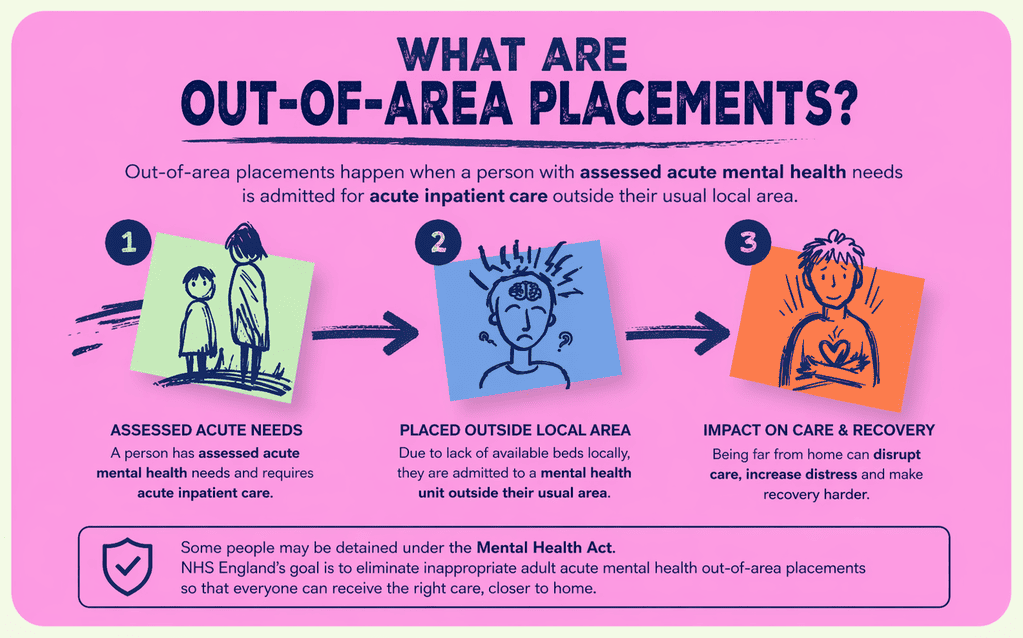
What Are Out-of-Area Placements?
Out-of-area placements happen when a person with assessed acute mental health needs is admitted for acute inpatient care outside their usual local network of mental health services. This can include admission to a general acute ward or, in some cases, a psychiatric intensive care unit when the right bed is not available closer to home.
In England, NHS guidance defines an adult acute out-of-area placement as admission to a unit that does not normally serve the person’s local catchment area, which can make regular contact with family, care co-ordinators, and local teams much harder.
Types of Services Involved
Out-of-area placements often involve a range of specialised services designed to support people with complex needs when appropriate support is not available locally. These placements can happen across different parts of the health and social care system, depending on the person’s needs, level of risk, and the type of support required at that time.
In many cases, people are moved between services over time, particularly if their needs change or if there are gaps in local provision.
Common settings where out-of-area placements may occur include:
- Secure services (low, medium, and high secure units) – for people who present significant risks to themselves or others and require care within secure environments, often under the Mental Health Act
- Forensic mental health services – supporting people who have come into contact with the criminal justice system and need specialist therapeutic and risk-managed care
- Specialist rehabilitation units – longer-term inpatient settings focused on recovery, skill-building, and gradual transition back to community living
- Child and Adolescent Mental Health Services (CAMHS) inpatient units – for children and young people requiring intensive mental health support that cannot be safely provided in the community
- Assessment and treatment units (ATUs) – short- to medium-term placements for people with learning disabilities and autistic people, usually during periods of increased distress or crisis
- Step-down or transition services – designed to support people moving from hospital settings back into community-based living, helping reduce the risk of readmission
- Crisis or emergency placements – rapid-response placements used when there is an immediate breakdown in support or a high-risk situation
Why Out-of-Area Placements Are a Growing Concern?
Out-of-area placements are especially concerning because they can disrupt continuity of care, delay discharge planning, and increase distress at a time when people may already be highly vulnerable, including those detained under the Mental Health Act.
NHS England has repeatedly stated the need to eliminate inappropriate adult acute mental health out-of-area placements, as being treated far from home is linked with negative experiences and adverse impact on people’s mental and physical wellbeing.
Increasing Demand and System Pressure
Demand for mental health services is growing, and the pressure is being felt across the whole system. More people are reaching a point where they need support, often with complex and layered needs that take time, consistency, and the right environment to understand properly.
At the same time, services are stretched – with limited bed availability, staffing challenges, and delays in finding the right support. This can lead to people being placed far from home, away from familiar faces, routines, and the sense of stability that can make such a difference during difficult moments.
Independent providers are increasingly part of this picture, helping to respond when local services cannot meet demand quickly enough. They often offer more flexible and specialist support, but their growing role also reflects wider gaps in the system.
For many people and families, this is not just about access to a placement, but about whether the support truly fits – whether it feels safe, consistent, and respectful of their needs. Keeping that focus matters, especially as systems continue to adapt under pressure.
How Distance Affects Continuity and Quality of Care?
When someone is placed far from home, care becomes harder to keep consistent. The people who know them best are no longer involved day to day, communication between teams takes more effort, and support can start to feel uneven. It also becomes harder to act quickly when something changes, which can affect how safe and understood a person feels.
- Different teams, different ways of working – no consistency in how support is delivered
- Family and carers are less involved – distance limits regular contact and input
- Slower communication – messages, updates, and concerns don’t move quickly
- Less understanding of the person – new teams don’t know what works yet
- Delays in decisions, reviews, and changes take longer to organise
- Missed early signs of distress – small changes go unnoticed without familiar people around
The Impact of Out-of-Area Placements
When someone is sent far from home, it changes everything around them. They lose daily contact with people who understand them, routines fall apart, and even small things that help them feel calm or safe disappear. Being in an unfamiliar place can increase distress, especially when support comes from people who are still trying to understand what works.
Families feel this just as strongly. Regular visits become difficult, sometimes impossible. They are less involved in decisions, less able to notice changes, and often feel pushed to the side. That distance builds frustration and worry over time, especially when updates are limited or delayed.
Carers and teams also feel the strain. They work across different services, often without clear communication or shared understanding. This might lead to missing important details, responses taking longer to get, and support becoming less joined-up.
What should feel coordinated starts to feel fragmented.
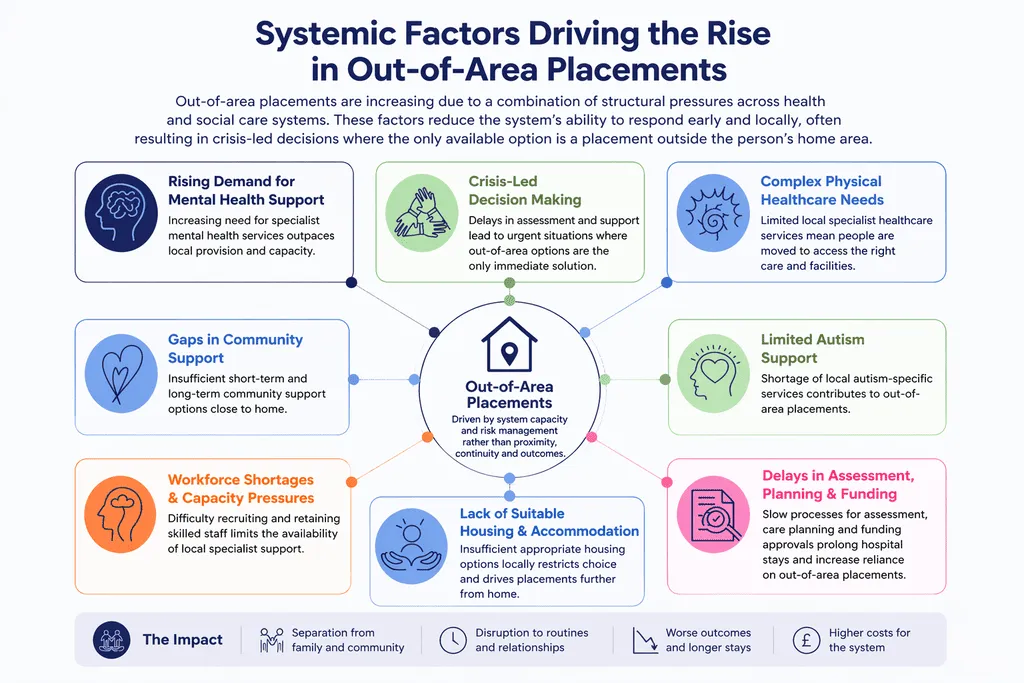
Systemic Factors Driving the Rise in Out-of-Area Placements
Out-of-area placements are increasing due to a convergence of structural pressures across health and social care systems. Demand for specialist support – particularly in learning disability, autism, and complex mental health – has grown faster than the development of local provision, leaving many areas without appropriate services.
At the same time, workforce shortages, limited access to suitable housing, and fragmented commissioning arrangements reduce the system’s ability to respond early and locally.
Delays in assessment, discharge planning, and funding approvals further compound the issue, often resulting in crisis-led decisions in which the only available option is placement outside the person’s home area.
Together, these factors create a pattern where placements are driven by system capacity and risk management rather than continuity of care, proximity to family, or long-term outcomes.
Lack of Local Specialist Services
In many areas, there are still not enough local specialist services to support people with complex mental health needs close to home. Gaps in provision across community mental health, learning disability, autism, and step-down support often mean that when a person is ready to leave hospital, there is nowhere suitable nearby for them to go. As a result, out-of-area placements can become the default rather than the last resort.
Workforce Shortages
Staffing pressures continue to affect the whole system, from inpatient settings to community mental health teams and specialist social care providers. When there are not enough experienced professionals with the right skills, it becomes harder to build stable support packages, respond early to changing needs, and prevent crisis. This can increase reliance on distant placements, especially for people who need highly tailored support.
Delays in Discharge and Care Planning
Even when a person is clinically ready to leave the hospital, delayed discharge is still a common problem. A lack of joined-up planning between hospitals, commissioners, housing, and community mental health services can slow down decisions and leave people waiting far longer than necessary for the right support to be arranged. These delays do not just affect flow through the system. They also prolong uncertainty for people and families who are ready for the next step.
What Needs to Change?
Better decisions depend on better information.
The care system needs a unified, coordinated system with information available for all people in need of care and support, people who are at risk of hospital admission, placement breakdown or out-of-area placements.
One reporting system – currently, we have at least five.
So, what really needs to change?
- Lack of unified systems – There are growing calls for a unified recording platform, shared data processes, and integrated IT systems. When systems fail to connect, it leads to delays, repeated work, and unnecessary duplication.
- Unclear roles and accountability – When roles aren’t clearly defined, collaboration breaks down because responsibility gets passed around and no one takes ownership.
- Capacity and workload pressures – Joint work slows down when teams don’t have time to meet or plan together. Without that, things don’t move properly – so lower caseloads and roles focused on joint working are needed.
- Inconsistent national guidance – Different interpretations of policy across areas create confusion and lead to inconsistent support, especially for people with complex needs.
- Unaligned funding – Without shared budgets or joint funding structures, agencies end up passing responsibility between each other instead of working together, which limits joined-up solutions.
Mandatory planning for vulnerable adults and children, with a named person responsible for keeping plans on track. Better working relationships. People understanding their role and the roles and responsibilities of other professionals, and people being accountable.
When providers submit clear, accurate, and up-to-date details, planning becomes more reliable. This includes thorough assessments, a realistic picture of day-to-day support, communication needs, risks, and what has or has not worked previously.
Without this, placements are often based on partial understanding, which increases the likelihood of breakdowns and delays. Consistent, high-quality information allows commissioners and teams to match support more appropriately and reduce unnecessary moves.
Investing in Local Community Services
In our white paper, commissioners consistently highlight the need to strengthen local community services as an urgent priority for investment.
Community-based provision was identified as the leading area for investment (82.5%), followed by training programmes (47.5%), AI tools to support care planning (35%), and remote monitoring (27.5%). This reflects a clear direction towards building capacity closer to home, where support can be more responsive and sustainable.
At the same time, commissioners describe structural gaps that continue to drive out-of-area placements.
“Lack of willingness to invest in purchasing property is leading to expensive out-of-borough placements.”
These insights show that the issue is not only demand, but how and where investment is made. Without local infrastructure, people are more likely to be placed further away, often in settings that do not reflect their long-term needs. Strengthening community services, alongside housing and step-up options, allows support to be built around people’s lives rather than relocating people to fit what is available.
“Lack of step-up accommodation – and long waiting lists for what does exist – often means people have to move into 24-hour residential settings while they wait for a supported living or extra-care place. This increases the risk of becoming institutionalised.”
Strengthening Integrated Care Systems
Strengthening integrated care systems means bringing the right people into decisions early and keeping them involved throughout planning, commissioning, and delivery. NHS England’s integrated care guidance describes ICSs as arrangements that require organisations to operate with partners, while The King’s Fund notes that place-based partnerships work best when NHS organisations, local authorities, voluntary sector partners, and communities shape priorities together.
In practice, that means commissioners, providers, carers, and multidisciplinary teams need to share information openly, align around a clear picture of need, and take joint responsibility for transitions and outcomes. Strong stakeholder engagement makes planning more realistic, reduces fragmentation, and helps systems build support around people locally rather than defaulting to disconnected or crisis-led decisions.
More Effective Discharge Planning
More effective discharge planning follows a defined process that brings together assessment, involvement, and preparation from the start:
- Early discharge planning from admission – clear timelines, shared responsibility, and coordination between hospital teams, commissioners, and providers.
- Active involvement of local service staff – engaged early to shape how support will work day to day and prepare before discharge.
- Comprehensive assessments – including needs assessment, risk assessment, communication assessment, and trauma-informed assessment to understand triggers, past experiences, and what supports emotional safety.
- Ongoing risk assessment – continuously updated and linked to real situations, not treated as a one-off document.
- Co-produced care planning – developed with the person, not for the person, reflecting routines, preferences, and what matters in daily life.
- Family involvement – families are actively included in planning, sharing insight, and helping shape consistent support.
- Building trust and relationships – early introductions to the support team, time to build familiarity, and consistent communication before discharge.
- Securing safe and stable community support – confirmed before discharge, including the right environment, consistent staffing, and continuity of support to avoid gaps or breakdown.
- Coordinated transition planning – all stakeholders aligned, with no last-minute arrangements or gaps in support.
Case Study
Nurseline Community Services supported a person who had spent 30 years in hospital to transition into the community safely and smoothly.
Lisa’s Transition Plan
Lisa spent nearly three decades in institutional care, far from her community. During this time, Lisa experienced complex mental health needs, faced significant challenges with self-care, and had limited control over her life, choices, and future.
First, an assessment and care plan development took place.
The care team included support workers, CPNs, PBS specialists, the transition team, a multimedia specialist, RMs, the registered manager, and the general manager. The team worked closely with Lisa and took part in ward rounds to understand and identify potential triggers for behaviour of concern.
Lisa actively contributed to developing her PBS plan, working together with the therapy team, RMs, and the hospital.
Phased transition strategy: In the initial phase, support workers shadowed hospital teams, and Lisa moved into one-to-one support. Through this process, Lisa built trust, which was essential for the transition.
See the full case study here.
The Role of Care Providers in Reducing Out-of- Area Placements
Reducing out-of-area placements depends on the quality of information shared at the very start. Care providers are central to this. Providers submit accurate information, and the accuracy, depth, and clarity of what is submitted about a person’s needs, risks, strengths, preferences, and support history directly influence placement decisions, timelines, and outcomes.
When information is detailed and reliable, commissioners and multidisciplinary teams can make informed decisions, avoid unsuitable placements, and reduce unnecessary delays. It also increases the likelihood of people being supported closer to home, in environments that reflect real needs rather than assumptions.
Accurate information supports safer transitions and more stable support arrangements. It allows teams to plan properly from the outset, instead of trying to correct gaps later. In practice, this places care providers at the centre of better planning, better matching, and more sustainable local support.
Supporting Transitions from Hospital to Home
- ~2,000+ people remain in inpatient settings despite being ready for discharge
- Over 50% of discharge delays are linked to a lack of community support, not clinical need
- Out-of-area placements often mean being far from family (100+ km)
- Delayed discharges directly affect patient flow and increase system pressure
Effective hospital-to-home transitions require a transparent and step-by-step process. All actions need to be carefully planned, all risks measured, and safety guaranteed.
What actually improves transitions:
- Early discharge planning (from the moment of admission)
- Strong stakeholder engagement (families, NHS providers, support providers)
- Regular pre-discharge visits to build familiarity and trust
- Preparation of the local environment before the move
- Clear handover to ensure continuity of care and support
What happens when this doesn’t work:
- People stay in the hospital longer than needed
- Moves happen in crisis, not through planning
- Higher risk of inappropriate out-of-area placements
- Support breaks down soon after discharge
Providing Specialist Community-Based Support
Strong local community mental health services change what support looks like day to day. Instead of people being moved away when things become difficult, support is built around them, where they already live, with people who know them.
This means moving beyond reactive care and building responsive, multidisciplinary support around each person – where psychological input, behavioural understanding, occupational therapy, and social support are coordinated, not fragmented.
This works when support is consistent and joined up. Carers, therapists, and wider teams share understanding, adapt support as needs change, and stay involved over time. There are regular check-ins, not just responses in crisis, and plans reflect how life actually looks – not just what is written on paper.
When local services are set up like this, fewer situations escalate to hospital admission. People keep their routines, stay connected to family, and experience more stability. Support becomes something that fits into life, rather than something that disrupts it.
Preventing Hospital Admissions
Preventing hospital admissions starts much earlier than the point of crisis. It relies on consistent, proactive support that recognises changes in a person’s wellbeing before they escalate.
This includes:
- Regular assessments
- Regular review and adaptation of care plans
- Clear understanding of triggers
- Responsive adjustments in day-to-day support
When carers and multidisciplinary teams share information openly and act on early signs – whether that’s increased anxiety, changes in behaviour, or withdrawal – there is a real opportunity to stabilise situations within the community. Psychological input, Positive Behaviour Support, and occupational therapy all contribute to building a clearer picture of what is happening and how support can adapt in real time.
Equally, preventing admissions depends on people having access to support that feels safe, familiar, and reliable. Strong relationships with carers, involvement of families, and continuity in support reduce uncertainty and distress, which are often at the root of escalation. Crisis is rarely sudden – it develops when needs are not fully understood or responded to. By strengthening local support, coordinating multidisciplinary input, and maintaining a consistent presence around each person, services can reduce avoidable admissions and support people to remain in environments where they feel understood and in control.
The Future: Moving Towards Localised Care
Across health and social care, there is a clear shift towards supporting people closer to home – driven by both system pressure and better outcomes. Out-of-area placements are costly, harder to oversee, and often disconnect people from their families and support networks.
In contrast, local placements allow funding to be used more effectively, strengthen safeguarding through closer oversight, and enable faster, more informed decision-making.
When a strong local network of services is in place – where psychological support, behavioural expertise, occupational therapy, and social care are coordinated – people are far more likely to remain stable, avoid unnecessary admissions, and receive support that reflects their actual needs.
Building Sustainable Community Models
Sustainable community models are built around consistent, well-coordinated support that allows people to make progress in environments they know and trust. When community care is structured properly – with psychological input, behavioural understanding, occupational therapy, and social support working together – it creates the conditions for stability and development over time.
Rather than responding only at the point of crisis, these models provide ongoing support that adapts as needs change, helping people maintain routines, strengthen skills, and move forward at their own pace. This kind of continuity makes progress possible, not as a one-off outcome, but as something that is sustained within everyday life.
Reducing Reliance on Institutional Care
How to reduce reliance on institutional care?
Reducing reliance on institutional care requires a structured and multi-faceted process that involves healthcare services, local authorities, people, their families, and reliable community care providers.
Whenever a person shows signs of distress and there is an anticipation of an upcoming crisis, immediate support is required. This involves person-centred care that understands the person’s true needs, rather than focusing only on diagnoses.
Early assessment and intervention play a key role here, as when care and support are proactive rather than reactive, there is a significantly reduced need for institutional care.
Urgent crisis response provides stabilisation and prevents further crisis escalation, helping to avoid potential hospital admissions. The right community care enables progress by creating capable environments where people can learn, grow, and become the best versions of themselves.
It also helps reduce dependence on restrictive settings by ensuring that support is delivered early, consistently, and in the right environment. When community support is responsive, coordinated, and built around the person, it creates stronger foundations for long-term progress and a better quality of life.
Bringing Care Closer to Home
For many people, staying connected to familiar surroundings, relationships, and routines can make a real difference in how they engage with further treatment and recovery. When care is delivered locally, it becomes easier to maintain family involvement, build trust with carers and teams, and create consistency across support. However, financial constraints continue to shape decisions, often limiting local options and leading to placements that prioritise availability over suitability. This can distance people from their support networks and make progress harder to sustain.
Care that is closer to home helps prevent placements that can put people at risk – where disconnection, unfamiliar environments, and lack of consistent support can lead to deterioration, unsafe situations, and harm to their wellbeing.
Addressing this requires significant stakeholder engagement, where healthcare services, local authorities, care providers, families, and people themselves are actively involved in planning and decision-making. When responsibility is shared and communication is clear, it becomes possible to design support that reflects real needs rather than system pressures. Investing in local, community-based provision allows care to adapt over time, reducing disruption and supporting more stable outcomes. In this way, bringing care closer to home becomes a practical, human-centred approach that supports continuity, dignity, and long-term progress.
Community Transitions From Hospital To Home with Nurseline Community Services
Nurseline Community Services provides comprehensive Community Transition Support (CTS) to ensure safe, well-planned transitions from hospital to home or community-based settings.

The CTS approach is centred on the person, with support tailored to individual needs, strengths, and circumstances. By working closely with social care professionals, local authorities, and families, the team helps ensure that the right support is in place at the right time, helping people regain stability, confidence, and a sense of control in their everyday lives. Discharge planning is approached as a coordinated process in which immediate needs and longer-term outcomes are considered together through a multidisciplinary approach to working.
Services are delivered across the UK, enabling people to access support closer to home, where continuity, familiarity, and connection can be maintained. The focus remains on creating stable, responsive support that adapts over time, reducing the risk of readmission and supporting sustainable progress within the community.
This approach is about creating the conditions for recovery to continue beyond hospital – within environments where people feel safe, understood, and supported to move forward.
We deliver services across the UK, and our offices are located in Bristol, Birmingham and Gloucester.
Contact us today, and let’s continue building the care we all want to see.